Horner’s Syndrome
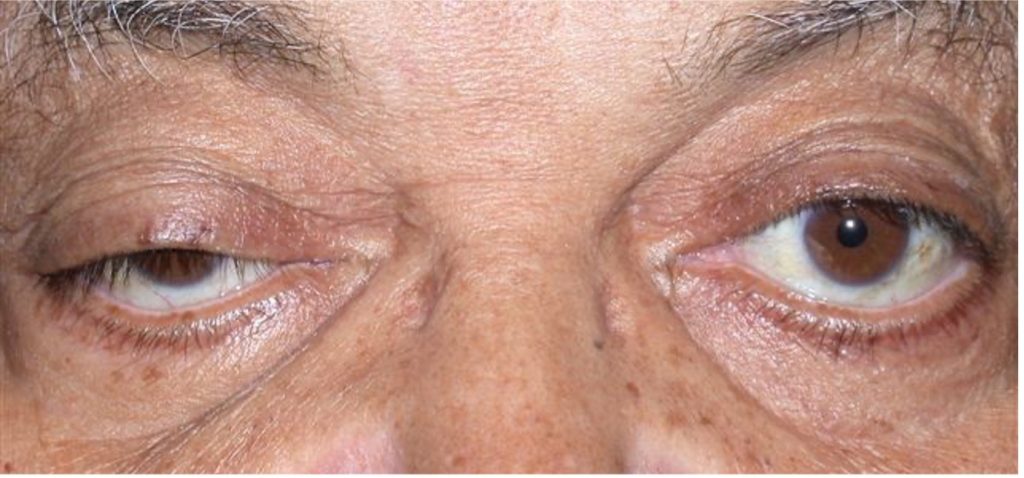
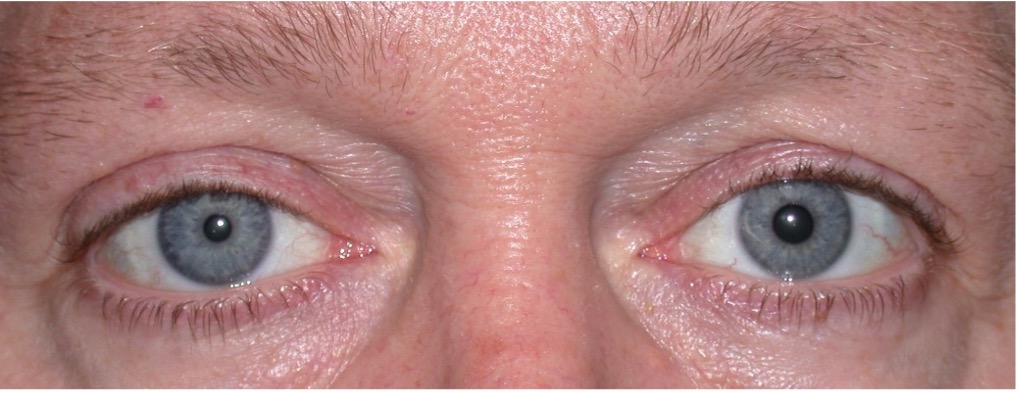
Horner’s Syndrome, or oculosympathetic palsy, is a condition in which the sympathetic nerve to the face and eye on one side is disrupted. The nerve originates in the brain, travels down the spinal cord, then back up through the chest, up the neck, then through the back of the eye socket and into the eye. The nerve primarily innervates an upper eyelid muscle, the pupil, and sweat glands on the face. If disrupted, the upper eyelid will droop, the pupil of that eye will be smaller, and there will be diminished sweating on that side of the face. Causes include anything that damages the nerve anywhere in its course, including a stroke, brain tumor, spinal cord disease, chest surgery, lung tumor, neck injury, or neck surgery. Its presence in children can be a sign of a malignant nerve tumor. Horner’s Syndrome can also be congenital, a result of migraine or cluster headaches, or may be of cause unknown.
There is no remedy for the damaged nerve, but if the eyelid droop is significant it can be lifted with surgery. The smaller pupil and lack of sweating on the face do not cause problems.
New onset drooping of an eyelid on one side may be a sign of a serious condition and should always be evaluated.